Angioplasty & Coronary Intervention
Angioplasty & Coronary Intervention
When the Heart Needs More Than Medication
Some cardiac conditions respond well to medication and lifestyle change. Others have reached a point where the arteries themselves need to be addressed directly. Narrowing or blockage in the coronary arteries reduces blood flow to the heart muscle, and when that narrowing is significant, the clinical answer is often coronary angiography followed by angioplasty.
At Oasis Clinics, the pathway from suspicion to intervention is managed as a single coordinated process. The cardiac workup, the decision to proceed, and the intervention itself are handled by the same clinical team, led by Dr. Amr Hassan Mostafa, one of Egypt’s most experienced interventional cardiologists, with procedures performed at a fully equipped partner facility adjacent to the clinic.
The Diagnostic Foundation: Coronary Angiography
Before any intervention, the anatomy of the coronary arteries needs to be clearly mapped. Coronary angiography is the gold standard for this. A thin catheter is introduced through the wrist or groin and guided to the coronary arteries, where contrast dye is injected and X-ray imaging captures the exact location, length, and severity of any narrowing or blockage.
Angiography answers the questions that non-invasive tests cannot fully resolve:
- Is there a blockage, and exactly where is it?
- How severe is the narrowing, and how many vessels are affected?
- Is the anatomy suitable for angioplasty, or is surgical bypass more appropriate?
- What stent size, length, and type will achieve the best result?
The angiogram is both a diagnostic procedure and the roadmap for everything that follows. In many cases, if the findings indicate a clear and treatable lesion, angioplasty is performed in the same session.
Angioplasty: Restoring Blood Flow
Angioplasty, formally known as percutaneous coronary intervention (PCI), is a minimally invasive procedure that opens narrowed or blocked coronary arteries without open-heart surgery. Through the same catheter access used for angiography, a guidewire is advanced past the blockage and a treatment catheter is delivered to the site.
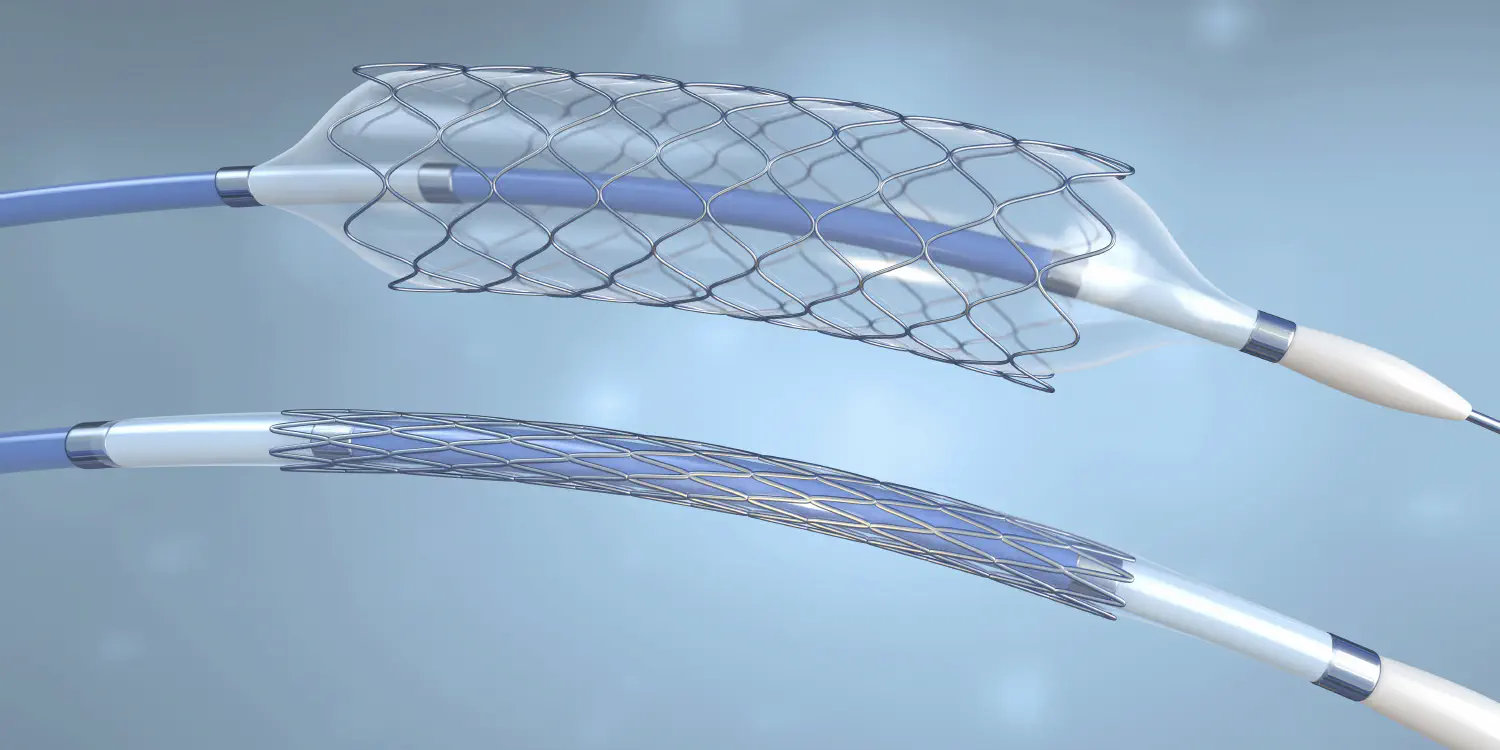
Balloon Angioplasty
A small balloon at the tip of the catheter is inflated at the site of the blockage, compressing the plaque against the artery wall and widening the vessel. In most cases, a stent is placed immediately after balloon dilation to maintain the opening.
Coronary Stenting
A stent is a small mesh tube that is deployed at the site of the treated blockage and left permanently in place to keep the artery open. It acts as a scaffold, preventing the artery from collapsing or re-narrowing after the balloon is removed.
Drug-Eluting Stents (Bio-Coated Stents)
Standard bare-metal stents carry a risk of re-narrowing (restenosis) as the artery heals around them. Drug-eluting stents are coated with a medication that is slowly released into the surrounding tissue, actively suppressing the cellular growth that leads to restenosis. They represent the current standard of care for most coronary stenting procedures and significantly reduce the need for repeat intervention.
The choice between bare-metal and drug-eluting stents, as well as stent dimensions, is determined by the angiographic findings, the vessel size, the lesion characteristics, and the patient’s overall clinical profile.
The Equipment
Coronary intervention requires imaging infrastructure that matches the precision of the procedure. The procedures coordinated through Oasis Clinics are performed using:
- High-definition digital fluoroscopy for real-time vessel imaging throughout the procedure
- Intravascular ultrasound (IVUS) where indicated, for detailed assessment of plaque composition and stent deployment
- Fractional flow reserve (FFR) measurement for functional assessment of borderline lesions, determining whether intervention is genuinely warranted
- A full range of contemporary stent platforms including latest-generation drug-eluting stents with biodegradable polymer coatings
The Pathway at Oasis Clinics
Step 1: Cardiac Consultation and Workup Everything begins at Oasis Clinics. The initial consultation with Dr. Amr Hassan Mostafa includes a full clinical history, ECG, echocardiogram, and relevant blood work. If non-invasive testing including stress testing or further imaging indicates significant coronary disease, the decision to proceed to angiography is made at this stage.
Step 2: Pre-Procedure Assessment Before the procedure, a complete pre-intervention assessment is carried out. This includes coagulation studies, renal function (contrast is used during the procedure and kidney function affects its safety), medication review, and patient preparation.
Step 3: The Procedure Coronary angiography and angioplasty are performed at a fully equipped partner facility located near Oasis Clinics, where Dr. Amr Hassan Mostafa operates as the lead interventional cardiologist. Patients are accompanied through the transition and remain under the care of the same team throughout.
Step 4: Post-Procedure Care and Follow-Up After the procedure, follow-up returns to Oasis Clinics. This includes wound site review, medication management (dual antiplatelet therapy is standard following stenting), echocardiographic assessment of cardiac function, and a cardiac rehabilitation plan where indicated.
Who Is a Candidate
Coronary angiography and angioplasty are considered for patients with:
- Stable angina that has not responded adequately to medical management
- Unstable angina or acute coronary syndrome requiring urgent assessment
- A positive stress test indicating significant ischemia
- Evidence of coronary artery disease on non-invasive imaging
- Prior stent or bypass surgery with recurrent symptoms suggesting restenosis or new disease
- Shortness of breath, chest tightness, or exertional symptoms where a coronary cause has not been excluded
Not every patient who undergoes angiography will proceed to angioplasty. In some cases, the findings indicate that medical management is sufficient, or that surgical bypass is a more appropriate option. The angiogram provides the information to make that determination with certainty.
Frequently Asked Questions
What is the difference between angiography and angioplasty? Angiography is the diagnostic procedure. It maps the coronary arteries using contrast dye and X-ray imaging to identify blockages. Angioplasty is the treatment that follows when a significant blockage is found: a balloon and usually a stent are used to open the artery and restore blood flow. In many cases both are performed in the same session, but the decision to proceed from diagnosis to treatment is made based on what the angiogram shows.
Is angioplasty open-heart surgery? No. Angioplasty is a minimally invasive catheter-based procedure. There is no surgical incision in the chest. Access is through a small puncture in the wrist or groin. Most patients are awake throughout, with local anesthesia at the access site. Recovery is significantly faster than open-heart surgery, and most patients are discharged within 24 to 48 hours.
What is a drug-eluting stent and why does it matter? A drug-eluting stent is coated with medication that is gradually released after implantation to prevent the artery from re-narrowing. Compared to older bare-metal stents, drug-eluting stents substantially reduce the rate of restenosis, which is the main reason patients sometimes needed repeat procedures after stenting. They are now the standard choice for most coronary interventions.
How long does the procedure take? A diagnostic angiogram typically takes 30 to 45 minutes. If angioplasty is performed in the same session, the total procedure time is usually between one and two hours depending on the complexity of the findings and the number of vessels treated.
Will I be awake during the procedure? Yes, in most cases. The procedure is performed under local anesthesia at the catheter access site, with sedation available if needed. Patients are generally comfortable throughout and can communicate with the team during the procedure.
What is recovery like after angioplasty? Most patients are discharged within 24 to 48 hours. Physical activity is restricted for a short period, and dual antiplatelet medication (typically aspirin and a second agent) is prescribed to prevent clotting around the stent. A follow-up plan is arranged before discharge and managed through Oasis Clinics.
When should I seek urgent assessment rather than a routine consultation? If you experience chest pain at rest, chest pain that is new, worsening, or not relieved by medication, or if you have had a previous cardiac event and are experiencing new symptoms, you should seek urgent assessment. Do not wait for a scheduled appointment.
Why does the procedure take place at a partner facility rather than at Oasis Clinics? Coronary angiography and angioplasty require a dedicated cardiac catheterization laboratory with fluoroscopy imaging and full emergency cardiac backup. The partner facility adjacent to Oasis Clinics has this infrastructure. The clinical team, led by Dr. Amr Hassan Mostafa, operates across both settings, and patients remain under the care of the same cardiologist throughout.
Is this suitable for patients who have already had a stent or bypass surgery? Yes. Patients with prior coronary intervention who develop recurrent symptoms may have restenosis within a previous stent or new disease in other vessels. Repeat angiography is the appropriate investigation, and angioplasty can be performed again where indicated.
What medications will I need after the procedure? Following stenting, dual antiplatelet therapy is standard, typically aspirin combined with a second antiplatelet agent such as clopidogrel or ticagrelor. The duration depends on the type of stent used and your overall clinical profile. Other cardiac medications will be reviewed and adjusted as part of the post-procedure follow-up at Oasis Clinics.